Conference Series Ltd conferences, 15th Annual Brain Death Congress during November 22-23, 2023 Paris, France aims to bring together leading academic scientists, researchers, specialists and research scholars to exchange and share their experiences and research results on all aspects of Brian Death, Brain Injury and Mental Illness. It also provides a premier interdisciplinary platform for researchers, practitioners and educators to present and discuss trends, the most recent innovations, and concerns as well as practical challenges encountered and solutions adopted in the fields of Brian Death, Brain Injury and Mental Illness.
Brain Death 2023 aims are to engage new audiences to participate in activities on the day Brian Death, Brain Injury and Mental Illness. Of course, we also want to reach existing followers of Neuro Science social media accounts, and to expand the global reach. Finally, this will be a great opportunity to explore as new science communication tool. We are now looking for people to contribute, and to help us make Neuroscience ‘go viral’!
Why to attend?
With members from around the world focused on learning about Neuroscience and its advances; this is your best opportunity to reach the largest assemblage of participants from the Brian Death, Brain Injury and Mental Illness. Conduct presentations, distribute information, meet with current and potential scientists, make a splash with new advancements and developments, and receive name recognition at this 2-day event. World-renowned speakers, the most recent techniques, developments, and the newest updates in Brain Death are hallmarks of this conference.
Target Audience:
-
Heads, Deans, Professors & University Faculty
-
Scientists and Researchers
-
Neuroscience Associations and Organizations
-
Laboratory members and Students working in this field
-
Physicians in the field of Neurology
-
Neurosurgeons
-
Nurse Practitioners (specially from critical care unit)
-
Business Intelligence Experts of Pharmaceutical Industries
Track 1: Brain Death
Brain death is determined by the complete and irreversible cessation of the whole brain activity including brain stem. The loss of consciousness leads to the respiratory and cardiopulmonary failure. Therefore, brain death results in all other organs’ death.
Track 2: Brain Injury
An Acquired Brain Injury (ABI) is an injury to the brain that is not hereditary, congenital, degenerative, or induced by birth trauma. Essentially, this type of brain injury is one that has occurred after birth. The injury results in a change to the brain's neuronal activity, which affects the physical integrity, metabolic activity, or functional ability of nerve cells in the brain. There are two types of acquired brain injury i.e., traumatic and non-traumatic.
Track 3: Brain Death Causes
While a person got an irreversible and catastrophic brain injury that causes the total cessation of the brain function which leads to brain death. Major causes of brain death are severe traumatic injury, cerebrovascular injury like stroke, anoxia due to heart attack, brain tumor etc. Brain infections, tumors, traumatic injury are responsible for brain swelling and for that brain loses its functions. Sometimes hypertension may cause bleeding in the brain that leads to brain death.
Track 4: Brain Death Diagnosis
The process of brain death determination and certification includes identification of physical examination findings which give a clear etiology of brain dysfunction. The diagnosis of brain death is clinically determined primarily. If the full clinical examinations including brain stem reflexes and apnea test are conclusively performed, then no other confirmatory tests are required. In some cases like cervical injuries or cardiovascular instability may cause misinterpretation of clinical tests’ result. In such case, a confirmatory test is necessary to verify the brain death properly. These confirmatory tests include angiography, cerebral arteriography, electroencephalography, nuclear brain scanning, transcranial Doppler ultrasonography etc. All the determination process should be done by at least two specialist physicians separately and all phases of determination should be recorded. Finally certification process should be done after completion of maintaining all records.
Track 5: Brain Death and Disorders of consciousness
Brain death and disorders of consciousness such as coma, vegetative state and minimally conscious state. Coma: A state of unconsciousness from the patient who cannot be aroused even with stimulation such a pressure on the supraorbital nerve, temporo- mandibular angle of the mandible, sternum, or nail bed. Vegetative state: This signifies an awake but unresponsive state, most of these patients were earlier comatose and a period of days or weeks emerges to an unresponsive state in which their eyelids are open, giving the appearance of wakefulness. This explains two inter-related paradoxes; the first paradox is the brain dead patient whose 'phenotype' betrays the ultimate futility and lack of sustainability of the state and the second paradox is that of patients who retain apparent higher levels of cognitive function but who may be misidentified as remaining in a vegetative state or one of the similar conditions formulated in the recently defined syndrome of cognitive motor dissociation.
Track 6: Brain Tumor
A brain tumor is an abnormal growth of cells inside the brain or skull. A primary brain tumor is an abnormal growth that starts in the brain and usually does not spread to other parts of the body. Primary brain tumors may be benign or malignant. Metastatic (secondary) brain tumors begin as cancer elsewhere in the body and spread to the brain. They form when cancer cells are carried in the blood stream. The most common cancers that spread to the brain are lung and breast.
Track 7: Coma vs. Brain Death
Individual in a state of coma is considered as alive, no matter how severe or prolonged. There is a chance to get back into the normal life for the coma patients as the patient is in reversible unconscious condition but brain continuously gives electrical impulse signal to rest of the body. In case of brain death patients, they are in irreversible unconscious condition i.e. complete and irreversible cessation. In case of vegetative state coma, the patient has recovered brain stem function but not higher cognitive abilities. If the vegetative state continues for more than one month then it is considered as persistent vegetative state which normally leads to brain death. Only in rare cases, patient with persistent vegetative coma state can recover full mental awareness.
Track 8: Brain Stem Stroke
A stroke happens once the blood offer to the brain is interrupted. The manner a stroke affects the brain depends on that a part of the brain suffers injury. Brain stem strokes will have advanced symptoms, and that they are tough to diagnose. Brain stem strokes can have complex symptoms, and they can be difficult to diagnose. If a stroke within the brain stem results from a clot, the quicker blood flow is restored during this essential space, the higher the possibilities for recovery. The risk factors for brain stem stroke are the same as for stroke in other areas of the brain: high blood pressure, diabetes, heart disease, atrial fibrillation, and smoking. Like strokes in other areas of the brain, brain stem strokes can be caused by a clot or a hemorrhage. There are rare cases, as Associate in Nursing injury to Associate in Nursing artery thanks to fulminant head or neck movements.
Track 9: Mental Illness
Mental health includes emotional, psychological, and social well-being. It affects how we think, feel, and act. It conjointly helps confirm however we have a tendency to handle stress, relate to others, and build decisions. Mental health is very important at each stage of life, from childhood and adolescence through adulthood. Over the course of your life, if you expertise psychological state issues, your thinking, mood, and behavior may well be affected. Many factors contribute to psychological state issues, as well as Biological factors, like genes or brain chemistry, Life experiences, like trauma or abuse, case history of psychological state issues. Mental health refers to our psychological feature, behavioral, and emotional upbeat - it's all regarding however we predict, feel, and behave. The term 'mental health' is typically accustomed to mean Associate in Nursing absence of a mental disturbance.
Track 10: Pediatrics Brain Diseases
Developmental Brain Injury and Disorders (DBD) occur prior to birth or in early childhood. They may be caused by genetic factors or can be brain injuries acquired through exposure to environmental factors (such as fetal alcohol spectrum disorder, infection, physical brain injury or drug addiction in the mother). DBD commonly affect the person throughout their entire lifetime and symptoms fall on a spectrum from high-functioning children and adults, to more mildly or severely affect individuals with intellectual disability and a variety of other common symptoms. Some children born with DBD can also have defects in other organ systems as part of a syndrome.
Track 11: Rehabilitation of Traumatic Brain Injury
Traumatic Brain Injury (TBI) occurs when an outside mechanical force is applied to the head and affects brain functioning. It can be caused by a blow to the head or a penetrating head injury or a rapid acceleration- deceleration event if the head has not been directly struck. Mostly common in a large group of disease causing acquired brain injuries.
Track 12: Clinical Evaluation of Brain Death
Clinical Evaluation of Brain Death is divided into two main categories they are Prerequisites and Neurologic Assessment. Prerequisites: Brain death is the absence of clinical brain function when the proximate cause is known demonstrably irreversible. Clinical or neuroimaging evidence of an acute catastrophe that is compatible with the clinical diagnosis of brain death. No drug intoxication or poisoning. Neurologic Assessment: Coma, Absence of brainstem reflexes and apnea test.
Track 13: Anoxic Brain Injury
Anoxic cerebrum damage is a kind of mental damage that isn't typically brought about by a hit to the head. Rather, anoxic mind damage happens when the cerebrum is denied oxygen. Left without oxygen for a really long time, neural cells start to kick the bucket through a procedure called apoptosis. What's more, however, cell passing is an ordinary piece of the human experience, when countless synapses at the same time bite the dust, patients can be left with decreased mind work. In the event that the oxygen hardship proceeds, anoxic cerebrum wounds may even wind up lethal.
Track 14: Nursing and Intensive Care practices
Caring of brain death diagnosed patient is the heaviest of duties for nurses. Due to stressors and complications, this is the biggest challenge of nursing in critical care unit. Nurses working in ICU must be knowledgeable about the brain death diagnosis and taking care of patients and their family especially when the patient is potential organ donor.
Track 15: Organ Donation and Complications
For the advancement in modern science and technology, organ donation is the greatest achievement by which an organ failure patient may get new life. Organ donors are of two types as living related donor and living non-related donor like brain death patient and cadaveric donor. After brain death, donated organs are kept viable by using ventilator or other supporting mechanisms until it will be transplanted. In case of brain death, patient can donate most of the organs. Critical care management of a potential donor patient is very crucial to maximize the number and the quality of the transplanted organs.
Brain death is the total and irreversible loss of all brain functions and the circumstance under which the donation of vital organs most commonly takes place. Brain death occurs when a person has a catastrophic brain injury leading to a total cessation of all brain function including the upper brain structure and brain stem. Brain death isn't a coma or persistent vegetative state. Brain death is decided within the hospital by one or a lot of physicians not related to a transplantation team.
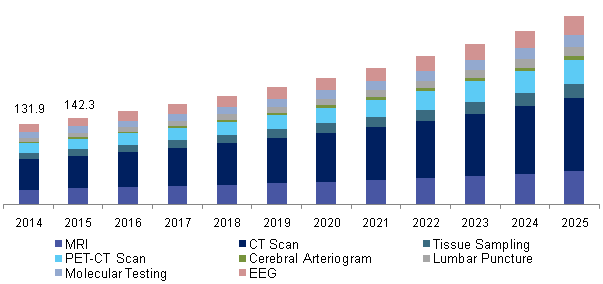
A brain-dead patient is meant to own no clinical proof of the brain perform upon physical examination. The examination exhibits no cranial nerve reflexes and no response to pain. The reflexes include no spontaneous respirations, oculocephalic reflex, pupillary response (fixed pupils), corneal reflex, and no response to the caloric reflex test. According to the World Health Organization estimates, neurological disorders are responsible for 4.5%-11% of all illnesses including low or high-income economies. This is far higher as compared to the number of respiratory ailments, gastrointestinal disorders, or cancers, and the burden is expected to increase further over the coming years.
The global market of dead identification and treatment is anticipated to grow at a CAGR of roughly 7% throughout the forecast amount 2017-2023.
The global Brain dead diagnosing and treatment market consists of states particularly America, Europe, Asia Pacific, and also the geographic area.
North America dominated the world brain dead diagnosing and treatment market as a result of the increasing tending expenditure. In the United States, If the patient is at or near death, the hospital must notify a transplant organization of the person’s details and maintain the patient while the patient is being evaluated for suitability as a donor. The patient is kept on ventilator support until the organs have been surgically removed. Furthermore, increased R&D activities and the concentration of major companies have fuelled the growth of the market in this region.
Europe holds the second position within the world dead diagnosing & treatment market as a result of the govt support for analysis & development and accessibility of funds for analysis. For instance, in countries such as Spain, Finland, Poland, Wales, Portugal, and France, everyone is automatically an organ donor after diagnosis of death on legally accepted criteria, although some jurisdictions such as Singapore, Spain, Wales, France, Czech Republic and Portugal allow opting out of the system. Elsewhere, consent from family members or next-of-kin may be mandatory for organ donation.
The Asia Pacific is that the fastest-growing dead diagnosing & treatment market as a result of the presence of quickly developing tending technology, increasing stressful life, and high healthcare expenditure. Moreover, the increasing patient population in countries such as New Zealand, Australia, drivers are asked upon application if they wish to be registered as an organ donor are likely to emerge because of the fastest-growing market across the world. Furthermore, increasing demand for quality devices intending is projected to steer the employment of advanced instrumentality, which, in turn, might increase the market growth during this region.
Furthermore in the Middle East & Africa, the spending on healthcare was also increased. The Middle East & Africa holds the least share of the market owing to less availability of funds, limited medical facilities, and deprived political conditions in Africa.

 Theresa D Hernandez
Theresa D Hernandez T. Chris Gamblin
T. Chris Gamblin Davide V Moretti
Davide V Moretti Wayne Carter
Wayne Carter Rocco de Filippis
Rocco de Filippis Alexander J.A. Groffen
Alexander J.A. Groffen Trevor Archer
Trevor Archer Yama Akbari
Yama Akbari Weidong Le
Weidong Le Michal Toborek
Michal Toborek Othman Ghribi
Othman Ghribi Frederik Willem Van Leeuwen
Frederik Willem Van Leeuwen Mustafa Nazıroğlu
Mustafa Nazıroğlu Piotr Lewczuk
Piotr Lewczuk